

{kind=link}

Poultry Postmortem in the Field: Practical Approach and Key Findings
Dr. Sakshi Patel
Assistant Professor, Department of Veterinary Pathology, Shourabh College of Veterinary Science, Kheda, RAJUVAS, Hindaun City, Rajasthan
Corresponding author email- sakshi.patel.vmk23@aau.ac.in
Abstract
Post-mortem examination is a vital diagnostic tool in poultry practice, particularly under field conditions where rapid disease identification is essential to prevent flock-level losses. This article outlines a systematic and practical approach to poultry necropsy, integrating step-wise examination techniques with interpretation of gross lesions. Beginning with external examination and progressing through body cavity opening to organ-wise evaluation, the procedure emphasizes correlation of findings with common infectious diseases of poultry. Characteristic lesions associated with major viral, bacterial, fungal and parasitic diseases are highlighted to aid field diagnosis. The approach described is simple, cost-effective and adaptable to field situations with minimal equipment, enabling veterinarians and students to make timely and informed decisions for disease control and prevention.
Keywords: Poultry post-mortem, Field diagnosis, Gross lesions, Lesion interpretation, Avian diseases
Introduction
Post-mortem examination (necropsy in animals and birds) is the systematic dissection of a carcass to determine the cause of death. In poultry, it is a crucial diagnostic tool, as diseases often occur at the flock level and may spread rapidly, leading to substantial economic losses in a short period.
This examination assists in identifying the cause of mortality, evaluating organ involvement and correlating lesions with clinical history and laboratory findings. Such integration supports accurate diagnosis, outbreak investigation and formulation of appropriate control and preventive measures.
In poultry production systems, disease occurrence is typically flock-oriented; therefore, a detailed flock history including management practices, vaccination status, mortality trends and clinical signs is essential for meaningful interpretation. Under field conditions, post-mortem examination becomes particularly valuable due to its rapid, practical and cost-effective nature, requiring minimal infrastructure. When performed in a systematic manner, it yields immediate gross findings that support prompt decision-making and help in limiting disease spread within the flock.
Post-Mortem Examination Under Field Conditions
Post-mortem examination in poultry follows a systematic protocol that integrates standard laboratory principles with field practicality. Ideally, necropsy should be performed soon after death to minimize post-mortem changes that may affect lesion interpretation. In a standard setup, instruments such as scissors, scalpel, forceps, bone cutters and collection materials are used. In field conditions, the procedure is simplified and basic instruments like sterilized scissors and forceps are usually sufficient when used carefully. However, biosafety remains essential and personal protective equipment such as gloves, apron, mask and cap should always be worn. Items like rings and watches should be avoided to maintain hygiene.
The carcass should be placed on a clean, well-lit (preferably sunlight) surface such as a tray, cloth, or paper for proper visualization. Systematic observation, palpation and incision are carried out in sequence, with careful recording of findings. Photographs taken at different stages help in accurate documentation and interpretation. A clear background and proper positioning are important to ensure good visualization of lesions and avoid diagnostic errors.
External Examination of the Carcass
For flock-level diagnosis, it is advisable to examine fresh carcasses along with moribund and a few apparently healthy birds to better understand disease expression within the flock. When live birds are selected for examination, humane methods such as cervical dislocation or other approved euthanasia techniques are followed.
Prior to post-mortem examination, the carcass is thoroughly washed with clean water to remove dirt and debris, facilitate feather handling and improve visibility of lesions while reducing the risk of sample contamination. After cleaning, a systematic external examination is performed, which often provides the earliest and most valuable diagnostic clues.
The comb and wattles are carefully examined for haemorrhage, oedema, swelling, or cyanosis (Figure 3), lesions commonly associated with systemic infections such as avian influenza (AI) and fowl cholera; the presence of shank haemorrhages (Figure 4) along with these findings further strengthens suspicion of AI. Ocular and nasal discharges are also recorded, as they are frequently associated with respiratory diseases including AI, infectious bronchitis (IB), infectious laryngotracheitis (ILT) and infectious coryza and gentle pressure near the beak may help express accumulated nasal exudate.
Attention is then given to vent area and droppings, where diarrhoea may be observed as an important clinical clue. Overall body condition is assessed by evaluating feather quality, skin integrity and presence of ectoparasites such as lice and mites, which may cause irritation, feather damage, anaemia and reduced performance. In some cases, skeletal condition may also be assessed by extending the legs; a rubbery consistency suggests underlying nutritional deficiency.
Skin Incision and Opening of Body Cavity
After completion of the external examination, the carcass is prepared for internal examination. The bird is positioned on its back with wings and legs extended to ensure stability on the examination surface. The skin between the thigh and abdominal region is first incised to expose the legs, followed by careful reflection of the skin. The hip joint is dislocated by separating the head of the femur from the acetabulum, allowing the carcass to lie flat and stable for better access.
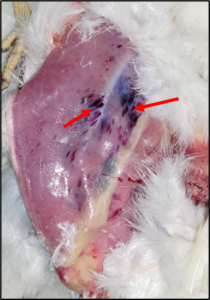
At this stage, the exposed thigh and breast muscles are carefully examined, as they often provide important diagnostic indications. The presence of large, blotch-like haemorrhages in these muscles is commonly associated with infectious bursal disease (IBD) (Figure 5), while similar but more severe and widespread muscle haemorrhages may be observed in systemic conditions such as AI. A pale carcass with intramuscular and subcutaneous haemorrhages is suggestive of chicken infectious anaemia (CIA), whereas a darkened and purplish discoloration of skin and underlying tissues may indicate fowl cholera. A sharply prominent keel bone is indicative of severe emaciation and is commonly seen in chronic debilitating conditions such as Marek’s disease (MD).
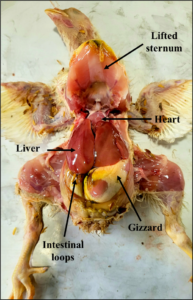
The abdominal muscles are incised gently up to the level of the rib cage, taking care to avoid deep or forceful cuts, as the lungs are firmly attached to the ribs and may be easily damaged. Following this, the sternum is lifted by cutting the muscles along both sides of the keel in field conditions, or by using bone cutters in standard procedures to cut through the ribs, thereby exposing the internal organs for examination. Once both thoracic and abdominal cavities are opened, the visceral organs are fully exposed, allowing systematic examination of each organ in situ (Figure 1).
Opening of Body Cavity and Organ Examination
The visceral organs are carefully evaluated in situ before or after removal for detailed examination. The liver is usually the first organ observed and is assessed for changes in size, colour and texture. A pale, enlarged and friable liver is suggestive of inclusion body hepatitis (IBH), while nodular lesions are commonly associated with MD and avian lymphoid leukosis (ALL). As the thoracic cavity is opened further, the heart and pericardial sac are examined; accumulation of straw-coloured fluid causing a distended appearance is characteristic of inclusion body hepatitis-hydropericardium syndrome (IBH-HPS), whereas fibrin deposition on the liver surface and pericarditis are commonly seen in colibacillosis. The heart is then incised to evaluate internal lesions.
For systematic examination, the entire visceral mass is often removed together by carefully cutting the oesophagus just above the proventriculus on the left side of the carcass and severing the cloacal attachments, ensuring intact removal of the proventriculus, gizzard, liver, spleen, pancreas and intestines. This facilitates detailed organ-wise examination.
Organ-wise Lesion Interpretation During Examination
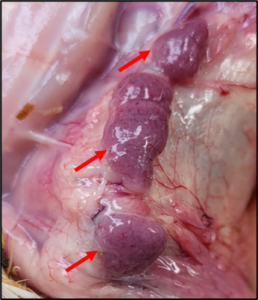
As organs are separated, characteristic lesions become evident. In the proventriculus, haemorrhages at gland tips (Figure 6) are strongly suggestive of Newcastle disease (ND), while haemorrhages at the proventriculus-gizzard junction may indicate infectious bursal disease. Similar lesions in AI are usually more widespread. The gizzard lining is normally easily separable; however, in necrotic enteritis it becomes firmly adherent due to severe mucosal damage.
The spleen is a small, oval to rounded organ, often described as pistachio-shaped, located in close association with the liver near the junction of the proventriculus and gizzard. It may be enlarged in viral infections, while nodular lesions in the liver, spleen, or kidneys suggest neoplastic conditions such as MD or avian leukosis. Pancreatic inflammation may also occur in IBH-HPS.
Intestinal lesions vary with the underlying disease process, with haemorrhages commonly observed in ND and AI, while necrosis is typically seen in necrotic enteritis. In coccidiosis, lesions are often site-specific; in caecal coccidiosis, the caeca contain haemorrhagic and caseous contents confined to these segments. Careful examination of the caecal tonsils is important, as haemorrhages (Figure 7) at this site are strongly associated with ND and AI. The intestines should also be examined for the presence of parasites, along with assessment of mucosal and serosal surfaces for any lesions.
The bursa of Fabricius, an important lymphoid organ located near the cloaca (Figure 2), is also examined. Haemorrhagic, oedematous, or caseous changes are characteristic of IBD and indicate severe immunosuppression.
The kidneys and lungs, being firmly attached to the body wall (Figure 2), are examined for swelling, congestion and urate deposition. Visceral uricosis is commonly observed in nephropathogenic IB, IBD and gout, indicating renal dysfunction.
Lungs and air sacs may show congestion or caseous exudates in respiratory diseases, while nodular lesions may be seen in aspergillosis. Special care is taken during kidney removal to avoid damage to the sciatic nerve, which may show enlargement in MD.
In adult birds, the reproductive system is also carefully examined. In males, the testes are two bean-shaped, pale-yellow organs located just anterior to the kidneys, while in immature females, ovarian follicles are observed in the same region (Figure 2). In mature females, well-developed ovarian follicles along with the left oviduct, which opens into the cloaca, are assessed for any pathological changes. Reproductive abnormalities such as reduced follicular development, regression, or oviductal changes are commonly associated with diseases like ND, IB and ILT, leading to decreased reproductive performance and poor egg production.
After removal of the abdominal and thoracic organs, examination proceeds to the neck region. The skin over the neck is incised and reflected to expose the underlying structures, and the nasal cavity is opened by making a transverse incision at the base of the beak near its attachment with the skin. The thymus, present as a chain of elongated lobes embedded in the subcutaneous tissue along both sides of the neck, is then examined for size and colour; congestion (Figure 8) is commonly observed in acute viral infections such as ND, IBD, and AI, while atrophy is characteristic of IBD and CIA. The trachea and oesophagus are subsequently assessed, and the trachea is opened along its entire length to detect any mucous plugs or caseous exudates, which are particularly suggestive of ILT. The oesophagus and surrounding structures are also examined for associated lesions. Subsequently, the skull is carefully opened by reflecting the skin over the cranium and upper mandible and the bone is gently cut to expose the brain for evaluation of neurological involvement. In suspected cases of CIA, the femur may also be examined to assess bone marrow condition, where fatty replacement of marrow is a characteristic finding indicating severe anaemia and immunosuppression.
Sample Collection and Biosafety
For confirmatory diagnosis, representative samples such as liver, spleen, intestine, trachea, and other affected tissues should be collected aseptically. Tissues intended for histopathological examination are preserved in 10% formalin, while samples for bacteriological and virological analysis should be collected in sterile containers and maintained under cold conditions. Care should be taken to minimize contamination during collection. After completion of the examination, proper disposal of the carcass and thorough disinfection of instruments and the working area are essential to prevent further spread of infection.
Conclusion
A systematic post-mortem examination in poultry is a valuable field-level diagnostic tool that provides immediate insights into disease conditions affecting the flock. By correlating gross lesions with clinical history and management factors, a veterinarian can arrive at a tentative diagnosis and initiate timely control measures. Proper collection and preservation of organs and samples for laboratory confirmation further strengthen diagnostic accuracy and support effective disease control and prevention.
 |
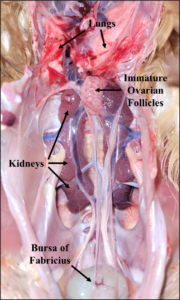 |
| Figure 1. Opened carcass with exposed visceral organs after reflection of sternum | Figure 2. Poultry carcass showing kidneys, lungs, ovarian follicles and bursa of Fabricius in situ |
 |
 |
| Figure 3. Severe cyanosis in comb and wattles | Figure 4. Haemorrhages in shanks |
 |
 |
| Figure 5. Haemorrhages in the thigh muscles | Figure 6. Pinpoint haemorrhages on the tips of proventricular glands |
 |
 |
| Figure 7. Haemorrhages in the caecal tonsils | Figure 8. Severe congestion of the thymus |
| Summary of External and Internal Gross Lesions in Major Poultry Diseases | ||||
| S.N. | Disease | External examination | Internal examination | |
| A. | Viral Diseases | |||
| 1. | Newcastle Disease (ND) (Ranikhet Disease) | Swollen, puffy head with watery, red, inflamed, closed eyes and greenish diarrhoea. | Pinpoint haemorrhages on proventricular gland tips, haemorrhages in caecal tonsils with intestinal ulceration and haemorrhagic enteritis, white necrotic splenic patches, tracheitis, lung congestion. Haemorrhage in ovarian follicles | |
| 2. | Infectious Bursal Disease (IBD) (Gumboro disease) | Haemorrhages in thigh and breast muscles, self-vent pecking, watery white diarrhoea | Swollen haemorrhagic bursa with gelatinous exudate or caseous mass (later atrophy), thymic atrophy and swollen kidneys with urate deposition | |
| 3. | Infectious Bronchitis (IB) | In adult layers: Misshapen eggs, thin or soft-shelled eggs, poor egg quality with watery albumen | Tracheal congestion with mucous, cheese-like exudate in the lower trachea, bronchi or air sacs and swollen, haemorrhagic kidneys with urate deposition (nephropathogenic form). Underdeveloped oviduct or egg-bound condition. | |
| 4. | Infectious Laryngotracheitis (ILT) | Watery, red, inflamed, closed eyes | Haemorrhagic and congested tracheitis with caseous plugs in the trachea | |
| 5. | Fowl Pox | Nodular (wart-like) pock lesions on comb and wattles with crusts on eyelids (dry form) | Diphtheritic membranes in the oral cavity and upper trachea (wet form) | |
| 6. | Avian Influenza (AI) | Marked cyanosis (bluish discoloration) of the comb and wattles, accompanied by head oedema and shank haemorrhages. | Severe congestion and haemorrhages in multiple visceral organs including proventriculus and muscles, along with tracheitis and pneumonia | |
| 7. | Marek’s Disease (MD) | Paralysis, unilateral leg extension, irregular pupils, blindness, emaciation with a prominent keel bone. | Enlarged sciatic nerves and liver enlargement with or without nodules, along with nodules in spleen, gonads and other organs | |
| 8. | Avian Lymphoid Leukosis (ALL) | Thickened bones with enlarged legs. | Enlarged liver with diffuse nodules, splenomegaly, bursal atrophy | |
| 9. | Inclusion Body Hepatitis-Hydropericardium Syndrome (IBH-HPS) | Enlarged, pale, haemorrhagic, friable liver with necrosis and mottling, along with straw-coloured fluid in the pericardial sac (hydropericardium) | ||
| 10. | Chicken Infectious Anaemia (CIA) | Pale carcass with intramuscular and skin haemorrhages | Atrophy of thymus, bursa, caecal tonsils, spleen and pale-yellow fatty bone marrow. | |
| B. | Bacterial Diseases | |||
| 1. | Colibacillosis | Fibrinous pericarditis and perihepatitis with fibrin on the liver surface, along with thickened air sacs containing foamy, purulent exudate. | ||
| 2. | Infectious Coryza | Moist feathers under the wings, Swelling of the head (puffy face) with watery eyes and nasal discharge | Sinusitis with fibrinopurulent or mucous (caseous) exudate and small nodules in air sacs. | |
| 3. | Pullorum Disease | White diarrhoea and joint swelling | Unabsorbed yolk sac, Enlarged liver with necrotic (gray) nodules, nodules in spleen, lungs, heart, gizzard and intestine, with caecal cores and raised intestinal plaques. In adults, irregular, cystic, deformed, pedunculated, discoloured ovary. | |
| 4. | Fowl Cholera | Skin darkened and purplish | Heart thickened and fibrinous; air sacs thickened with foamy exudate; liver enlarged, darkened with haemorrhages, fibrin on surface and necrotic foci. | |
| 5. | Fowl Typhoid | _ | Enlarged, friable liver with a copper-coloured (metallic) sheen, inflammation of caecum, spleen, lungs and peritoneum in chicks; in adults, oophoritis with hard, shrunken egg follicles, along with salpingitis, orchitis and peritonitis | |
| 6. | Necrotic Enteritis | _ | Swollen, enlarged proventriculus and gizzard with eroded lining that does not peel off; small intestine markedly thickened with necrosis, showing a “Turkish towel” appearance. | |
| 7. | Tuberculosis | Emaciation, dehydration | Granulomatous nodules in liver, spleen, intestines | |
| C. | Mycoplasma | |||
| 1. | Chronic Respiratory Disease (CRD) | _ | Mucus mixed with blood in trachea, thickened air sacs with foamy exudate and fibrinous pericarditis with fibrin deposition on liver surface. | |
| D. | Fungal Disease | |||
| 1. | Aspergillosis (brooder pneumonia) | _ | Mouldy nodules in the nasal passages, trachea, air sacs and lungs, with lung nodules showing dirty grey-yellow cheesy exudate, along with yellowish discoloration of the liver. | |
| E. | Parasitic Diseases | |||
| 1. | Coccidiosis | Dehydration | Caecal coccidiosis: caeca filled with red, dirty exudate and cheese-like cores; intestinal coccidiosis: ballooning of affected intestine with thickened swelling, bloody exudate and pinpoint haemorrhages. | |
| 2. | Lice, mites | Loss of feathers, lice or mite eggs deposits at the base of shafts | ||
| 3. | Intestinal parasites (Ascaridia galli, Heterakis gallinarum, Raillietina, Davainea) | Emaciation, anaemia and diarrhoea. | Parasites in the intestinal lumen with mucosal thickening, haemorrhages, necrosis and enteritis | |
NB-ALL THE PHOTOGRAPHS HAS BEEN PROVIDED BY AUTHOR FOR KNOWLEDGE PURPOSE.
Reference
Vegad, J. L. (2018). Poultry diseases: A guide for farmers and poultry professionals (2nd ed.). CBS Publishers & Distributors, India.
Sastry, G. A. (2019). Veterinary pathology (7th ed.). CBS Publishers & Distributors, India.
https://www.basu.org.in/wpcontent/uploads/2020/06/Post_mortem_examination_of_birds_Part_1.pdf
Kalai, K. (2024). Post mortem examination of poultry birds with important gross lesions and sample collection during postmortem for laboratory tests. ResearchGate.