

{kind=link}

Compiled & shared by-DR Uday Kumar, Veterinary Surgeon,Patna
“Dystocia refers to a difficult birth due to either a protracted natural birth or a severe or protracted assisted extraction. It is associated with unacceptably high levels of pain”
In general, dystocia is more frequent in heifers than in multiparous cows and delivery for a heifer is believed to be more painful and stressful. This is due not only to the heifer’s lack of experience, but also to the fact that calving tends to take longer in heifers than in multiparous cows. It is also accompanied by a more pronounced inflammatory response and a slower postpartum recovery
In cows, calving usually lasts between 30 minutes and 4 hours from the time the amnion begins to protrude through the vulva to the expulsion of the calf. A calving is considered dystocic if it is excessively protracted or if severe assistance is required to extract the calf.
The two main causes of dystocia in cows are disproportion between the size of the foetus and the diameter of the pelvis (more common in heifers) and malpresentation of the foetus (more common in multiparous cows). Several factors, such as Cervical stenosis, uterine inertia , the dam’s diet or the breed of the bull, can affect the risk of dystocia.But in field level generally we come across the case of incomplete cervical dilation and uterine inertia.
Amongst all domestic animals, cattle and buffalo are considered the species in which the incidence of dystocia appears to be highest.
Causes of Dystocia in Cows and Buffaloes———
The causes of dystocia are generally classified into the maternal and fetal causes . Buffaloes are known to have greater incidence of maternal dystocia. As we know ,buffalo generally have fewer problems in dilation of the birth canal compared to cattle and there is a greater incidence of uterine torsion in buffaloes. The incidence of fetal monstrosities is higher in the buffalo
Maternal Causes of Dystocia———–
The maternal causes of dystocia are considered to be arising either because of the constriction/obstruction of the birth canal or due to a deficiency of the maternal expulsive force .
CONSTRICTION/OBSTRUCTION OF THE BIRTH CANAL———-
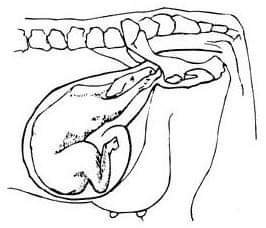
The constriction/obstruction of the birth canal can result in maternal dystocia and can be due to pelvic abnormalities, vulvar or vaginal stenosis, neoplasms of the vagina and vulva, vaginal cystocoele, incomplete cervical dilation, uterine torsion and ventral displacement of the uterus. An uncommon cause of constriction of birth canal is carcinoma of urinary bladder with metastasis in cervix.
1. Pelvic Abnormalities——
Pelvic abnormalities of the mother that can result in dystocia include small size of the pelvis , pelvic deformities or exostoses , osteomalacia and hypoplasia of vagina and vulva . Breeding of heifers at too young an age, breeding of poorly grown heifers, or breeding of heifers and cows that had pelvic fractures can result in a smaller pelvis of the mother culminating in dystocia at parturition. Breeding of small sized breeds of cattle or buffaloes with breeds of larger size can result in fetuses of bigger size being obstructed at the small sized pelvis of the mother. Rarely, the cause of small bony pelvis is sacral luxation or displacement . Other causes described include twins and intra pelvic hemorrhage . However, pelvic fractures and exostoses are considered to be uncommon as a cause of dystocia in large animals . An inadequate sized pelvis is a frequent cause of dystocia in the bovine primipara . Narrow pelvis is known to be a cause of dystocia in the cows /buffalo . The incidence of narrow pelvis has been recorded to be 12 percent.
Clinical Signs————-
Usually, there is a lack of progress in the second stage of labor. If the fetus is able to enter the pelvis partially, severe non-progressive straining occurs. If the fetus is too large, then there is no progress in delivery subsequent to first stage of labor. Vaginal examination must be done to compare the fetal and pelvic size. Any previous fractures can be ascertained by the presence of calluses.
Management of Dystocia——
If by palpation, it is felt that the fetus can pass through the birth canal with assistance, traction must be applied on the fetus after plenty of lubrication. However, excessive traction in a narrow birth canal is not advisable. It is better to opt for a caesarean section if the birth canal is too narrow, or it is coupled with fetal postural abnormality.
2. Incomplete Cervical Dilation—–
The dilation of the cervix at the time of delivery of fetus is essential for the easy passage of the fetus. A wide variety of changes in the hormonal milieu enzymatic loosening of fibrous strands by elevated collagenase and the physical forces of the uterine contractions and fetal mass are considered to be responsible to effect sufficient dilatation of the cervix during parturition in the cow and buffalo . An activation of inflammatory network is considered to play an important role in the progress of cervical dilation . An in crease in inflammatory cytokines during parturition is known to effect dilation as is the interplay of hormones. In buffaloes, however, cervical non-dilation is rare. Animals with delivery problems associated with the cervix are those that had already delivered many calves . Cervical non-dilation can occur because of the failure of any of the mechanisms responsible for dilation described above or spasm of the cervical muscles or some other poorly understood mechanisms and results in dystocia.
Clinical Signs———
When the cervix is fully dilated, it is not palpable as a separate structure and is continuous with the vagina. Incompletely dilated or undilated cervix is palpable through per rectum examination. By examination per vaginum only a finger or two can be inserted in a partially dilated cervix. Parts of fetus or the water bags can sometimes be palpated at the cervix.
Management of Dystocia———–
Attempts can be made to dilate the cervix manually if possible using sponge tents and local anesthetics , but because the cervix has many annular rings it is often not possible to dilate the bovine cervix manually. If the fetus is present in the birth canal gentle traction over long periods can sometimes dilate the cervix, but excessive traction is not advisable. It sometimes happens that a maldisposed fetus present in a previously dilated birth canal becomes tightly impacted because of continued uterine contractions without fetal delivery. An obstetrician must differentiate such a case from incomplete cervical dilation. If the cervix remains closed, the fetus is live and its fetal membranes are intact, it is suggested to wait for 30 minutes to allow time for natural dilation. A deficiency of estrogen is considered to be one important cause of failure of cervical dilation , hence, injection of estrogens like estradiol valerate 20 – 30 mg im can be helpful, however, estrogen should be given with care in a completely closed cervix because of the dangers of uterine rupture that may follow because of violent contractions. Likewise, injections of oxytocin 20 – 40 IU, iv or im can be given to promote uterine contraction to effect cervical dilation when it is partially dilated. When the legs of a putrefied dead, fetus are present in the birth canal and the fetus cannot come out because of incompletely dilated cervix, we suggest partial cervicotomy instead of a cesarean. One or two cuts applied on the cervix are usually sufficient to deliver the calf. We advice potent analgesics like valethamate bromide (Inj. Epidosin TTK Pharma, India) at the dose rate of up to 500 mg im or iv is of limited value in dilating a closed bovine cervix at term. β2 adrenergic drugs like isoxsuprine at doses of 200 – 300 mg iv or 0.3 mg iv clenbuterol have been suggested to relax the entire genital tract including the cervix but may not be always helpful because of the complex mechanism that is responsible for cervical dilation which largely remains poorly understood. Moreover, the β2 adrenergic drugs would reduce uterine contractions and hence delay parturition. Caesarean section appears to be the best resort when all attempts at cervical dilation have failed. Use of relaxin as a cervical ripening agent and its use for inducing labor in human subjects still remain unclear and hence, its use in animal therapy is out of question because of the high cost.
. FAILURE OF THE EXPULSIVE FORCES———–
Failure of expulsive forces could result because of the failure of abdominal or uterine expulsive forces. The condition where the uterine expulsive forces fail to deliver a fetus is known as uterine inertia. The uterus quietens and the progression of the fetus out of the birth canal does not follow because of lack of contractions in the uterus. Uterine inertia is classified conventionally into primary and secondary uterine inertia
Primary Uterine Inertia———
In this condition, although the cervical dilation occurs and the fetus is in normal presentation, position and posture but it is not delivered due to lack of uterine contractions. The process of birth begins but do not continue into second sage labor. The most common cause of primary uterine inertia in dairy cows and buffaloes is considered to be hypocalcaemia, with the animal showing signs of milk fever as calving is about to begin. Over distension of the uterus because of dropsical fetal conditions, general debility and environmental disturbances are other causes. A few of the less common causes include inherited weakness of uterine muscle, toxic infections, myometrial degeneration, senility and nervousness. The incidence of uterine inertia is known to be 5.9 percent . Therapy for dystocia management includes intravenous therapy with calcium borogluconate and 15 – 20 I.U of oxytocin IM or IV. When the cause is calcium deficiency animals will respond favorably and parturition process would begin. The fetus can be delivered after some time spontaneously or with little assistance. An injection of oxytocin must be given after removal of fetus to aid in uterine involution and placental expulsion.
Secondary Uterine Inertia————
Secondary uterine inertia occurs due to exhaustion as a result of dystocia . When the uterine musculature becomes exhausted subsequent to failure of delivery of a maldisposed or oversized fetus or due to obstruction in the birth canal, then the condition is known as secondary uterine inertia. The contractions in the uterus then stop or become weak and transient. The animal shows no progress in parturition after the second stage of labor. The fetal membranes are ruptured and the cervix dilated. If dystocia is prolonged without fetal delivery, the fetal fluids are expelled out and the uterus contracts tightly around the fetus. It is necessary to correct the primary cause of dystocia and deliver the fetus. Doses of oxytocin must be given after fetal delivery to regain uterine contractility. Secondary uterine inertia invariably results in retention of the placenta.
Steps in handling dystocia —-
1. After observing a delay in delivery, a pelvic examination should be done to determine the extent of cervical dilation. It should be dilated enough to allow easy passage of the fetus.
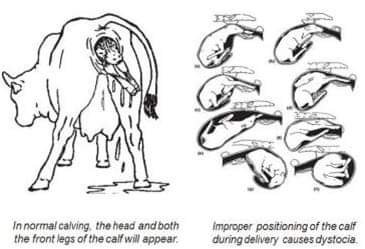
2. Determine the position of the fetus (Figures 1 and 2). If it is in an abnormal position, experience and judgement must be used to determine if a correction can be made or if professional help should be summoned.
3. Examine the size of the calf relative to the birth canal. A large calf forced through a small pelvic opening may result in death of the calf and injury (including paralysis) to the cow. If this examination is made when the head and front feet are still in the birth canal, the opportunity for a successful caesarean section exists.
4. If the examination indicates a dry fetus and birth canal, additional lubrication is needed. Use a commercial obstetrical lubricant (methyl-cellulose product) or petrolatum (Vaseline®). Do not use soap as it is irritating to the vaginal membranes, causes inflammation and swelling of the reproductive tract and can result in delayed return to estrus and lower conception rates.
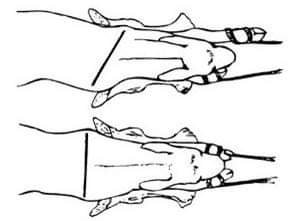
5. Attach the obstetrical (pulling) chains to the front legs of the calf, placing the loop of each chain around each leg. Placement of the chains should be around the pastern (below the dewclaw and above the hooves) with the looped chain on top of the hooves. Careful attention to this placement when pulling on the chains will generally result in the least amount of damage to the calf. If the chains are allowed to become slack and/or excessive force is applied, the chain may damage the hooves. Placing the chains above the fetlocks (above the dewclaws) with a half-hitch around the pastern can result in broken front leg(s).
6. Attach the obstetrical handles and pull gently, making sure the chains have not slipped. Although some calves can be delivered by pulling both legs evenly, it’s usually best to alternately pull on one leg and then the other a few inches at a time (Figure 3). Once the legs are “walked out” in this manner, the shoulders are allowed to pass through the pelvic opening one at a time. If the shoulders should happen to “lock” at the opening, apply traction to the calf’s head by attaching a chain around the poll and through the mouth. This traction will reduce compaction of the head against the sacrum (top of the birth canal) and reduce the dimensions of the shoulder and chest region.
7. The chance of uterine or cervical lacerations and tears is greatest when the calf’s head and shoulders come through the birth canal. Such damage may lead to infections and future reproductive problems. Since pressure dilates the birth canal, damage can usually be prevented if traction is applied gradually. Gradual application of traction also helps prevent damage to the cow if assistance happens to be given too early, because very slow traction will not interfere with normal dilation of the cervix.
8. Once the head and shoulders are exposed, rotate the calf a quarter of a turn to aid in the hips entering the pelvic canal. If this does not allow delivery, pull the calf downward at a 45-degree angle, or nearly parallel with the rear legs of the cow.
9. “Hip lock” can be a problem serious enough to cause loss of the calf. If it happens in a cow lying down, push the fetus back a short distance and rotate the calf a quarter turn, then apply traction to the front legs in a direction toward the cow’s flank or side. This rotates the calf enough so one hip bone goes through the pelvic opening ahead of the other. If you are unable to repel or rotate the calf, place the calf’s legs between the cow’s hind legs and pull forward. If delivery is delayed, make sure the calf begins breathing normally as the umbilical cord will be pinched closed.
10. All posterior (rear feet first) presentations should be considered an emergency, because the umbilical cord is pinched between the fetus and pelvis early in the delivery. This means blood circulation is slowed, and the fetus may die or sustain brain damage unless delivery is rapid.
11. Attach the obstetrical chains above the fetlock joint and be sure the birth canal is adequately lubricated, since extraction is against the normal direction of hair growth. A posterior delivery is usually eased by alternating traction on the rear legs and by rotating the fetus about a quarter of a turn to take advantage of the greatest diameter of the cow’s pelvis. If delivery proves extremely difficult, a caesarean section is probably necessary and should not be delayed.
12. Only an experienced herdsman or veterinarian should use mechanical calf pullers. If used incorrectly, permanent damage can occur to both calf and cow.
13. Correcting abnormal presentations other than a leg or head turned back usually requires professional help. For instance, a fetus that is upside down may be in that position because the uterus or fetus is rotated.
Management tips in dystocia———
1. Minimise situations liable to cause chronic stress, such as competition for food, water or a place to lie down. Ideally, prepartum pens should include a resting area equivalent to 11m2/cow and a feeding area big enough for all cows to feed at the same time (minimum of 0.76 m of feeder/cow). Additionally, each pen should have at least two water points.
2. The cow should be monitored once an hour from the onset of the first stage of calving. Intervention is only necessary if any stage of the calving process is excessively protracted and/or if atypical behaviour, or normal behaviour with abnormal frequencies, is observed.
3. Individual calving stalls should be arranged so that the cows within can make eye contact with other cows. This enables efficient monitoring of the calving, as well as proper expression of maternal behaviours in post-parturient dams. Individual stalls should have a surface area of at least 12m2, be fitted with straw bedding or sand, and be hygienic.
4. Group calving pens should never hold more than 30 cows each and should be designed to allow cows in labour to be separated without having to be removed from the pen.
5. Dams should be allowed to lick and ingest the amniotic fluid on the calf. Not only does this behaviour increase the calf’s vigour, it also helps to reduce the pain caused by the calving in the dam since the amniotic fluid contains certain compounds that enhance the analgesic action of endogenous opioids.
NB—-
Cleanliness cannot be overemphasized. Introduction of bacteria by equipment or arms of the person assisting with the calving may reduce fertility of the cow by delaying return to estrus and lowering conception. Equipment needs are two clean buckets, soap (for cleaning the cow), disinfectant, obstetrical lubricant, paper towels, calving chains and handles and plastic sleeves. Have water in both buckets — disinfectant is added to the second bucket. Place the calving chains and handles in the disinfectant solution.
Restrain the cow with head catch or halter. Tie the tail with light twine to the neck of the cow. Scrub the perineal area (around the anus and vulva) and the tail with soapy water. Pour water from the bucket to rinse the area. Do not dip dirty towels back into the bucket. When the area is clean, dry with paper towels. Use the remainder of the water in the first bucket to wash your hands and arms. If possible use plastic sleeves on initial examination. This may prevent contact with abortion-causing organisms that can infect humans. Apply an obstetrical lubricant to the sleeves. If extensive manipulation of the fetus is needed, the gloves may be removed since they tear easily.
Postpartum care——–
In case of caesarean section or dystocia, use of non-steroidal anti-inflammatory drugs (NSAIDs), alpha-2-agonists (such as xylazine) and/or local anaesthesia (procaine or lidocaine) is recommended. In the case of normal calvings, the administration of an NSAID following parturition can reduce pain and inflammation, improve health and welfare, and help to maintain or increase fertility and milk yield. Scientific data on the impact of analgesics following calving in cows is however limited and often contradictory.
Summary of calving management recommendations—-
1. Observe the herd closely during calving season, especially first-calf heifers because they will require the most assistance.
2. Have the proper equipment and facilities available prior to calving and in clean, working order.
3. Give assistance during delivery or call a veterinarian when needed. Do not wait more than a few hours after labor begins to act.
4. Correct any abnormal fetal positions in the early stages of delivery.
5. When pulling a calf, loop the chain or rope around the pastern. Apply gentle traction on one leg at a time to facilitate passage of the shoulders through the birth canal.
6. Remove mucus from the calf’s nose and mouth immediately after birth. If the calf does not start to breathe normally, tickle the nostrils, hold it up by the hind legs and shake it, or apply artificial respiration with a piece of hose or by alternating pressure and release on the rib cage.
7. Disinfect the navel cord with iodine to prevent infection. Make sure the calf nurses within an hour after birth or give colostrum to weak calves.
Keep birth weight and ease-of-calving records to identify those sires and dams responsible for calving problems. This information is especially important for selecting sires to breed yearling heifers. When possible, cull those females with a history of calving problems and avoid selecting replacement heifers from such cows. Table 2 shows a simple calving-ease scoring system
Reference:On request